Unraveling the Enigma of SSRIs: How Do They Work, and Do They Really?
SSRIS, or Selective Serotonin Reuptake Inhibitors, are a type of psychiatric drugs used to treat symptoms of depression and anxiety, or depressive and anxiety disorders. They are the most commonly prescribed antidepressants, and first began being used clinically in the late 1980s. The first ever SSRI, fluoxetine, was cleared for prescription usage in the United States in 1988, and paved the way for a new, much more reliable form of antidepressants. As of 2018, it is estimated that 13.2% of Americans above the age of 12 are on some form of SSRIS. The question is, what are they, really, and how do they work?
It’s important to first understand the Serotonin Hypothesis of Depression. This hypothesis states that low levels of serotonin (a neurotransmitter related to mood, sleep, digestion, and much more) in the brain, or an inability to process serotonin correctly, is the leading cause of depression. Within this hypothesis lays the groundwork for SSRIS; the theory being that increasing serotonin in the brain lowers symptoms of depression. Therewithal, it is incredibly difficult for scientists to measure serotonin levels, as when done through bodily fluids, such as blood, urine, or cerebrospinal fluid, deficits do not appear, even when the person has been clearly diagnosed with depression. This is because neurotransmitter levels in the brain are extremely localized, and therefore not well reflected by levels throughout the rest of the body. This makes it difficult for scientists to objectively ‘prove’ the serotonin hypothesis, and as of 2022, many psychiatrists no longer accept the serotonin hypothesis, claiming there is no direct correlation between serotonin levels and depression. But, if the serotonin hypothesis is false, why are SSRIS so commonly used, and do they really work?
Here’s what we do know. After a few doses of an SSRI, serotonin levels in the brain increase. This happens because the SSRI blocks the reabsorption (or reuptake) of serotonin into the neurons, allowing the neurotransmitter to better send messages between neurons. SSRIS are classified as selective because they only block the reabsorption of serotonin, and not of other neurotransmitters. If the SSRI works properly, the patient should see decreased symptoms of depression within the first two weeks to a month. And that’s it. That’s how they work. It seems quite simple, and foolproof, but many psychologists have begun to find holes in the argument for this.
Research done by Moncrieff et al includes compelling data suggesting that there is no consistent evidence linking lowered serotonin concentration or activity to depression. They therefore suggest it is “time to acknowledge the serotonin theory of depression is not empirically substantiated.” This leads many to question the effectiveness of SSRIS. But how could that be? For the most part, patients who use SSRIS report their symptoms of depression and anxiety decreasing significantly, as well as their mood stabilizing. It is possible that this is partially because of a placebo effect, which is when a person’s belief in the treatments is what is causing their improvement, and not the treatment itself. It is also possible that researchers claims do not hold as much truth as they believe. Despite there clearly being evidence of a lack of a correlation, there is also decades worth of evidence that SSRIS do work.
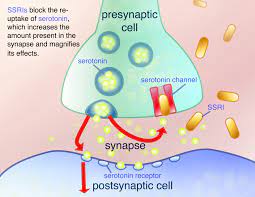
Image from: https://www.google.com/url?sa=i&url=https%3A%2F%2Fhopes.stanford.edu%2Fssris%2
Furthermore, it is important to note that we do not understand everything about SSRIS. The brain, and therefore, psychiatric medications, are incredibly complex. We tend to find that there isn’t just one answer to the psychology questions we seek, especially when considering that everyone is different, and there are lots of things we still don’t know about the brain. Psychiatrists and psychologists alike do not suggest stopping SSRIS if you are on one, especially not without consulting your physician. As research continues, we hope to find more of the answers we seek, although it’s hard to say what the near future holds for current theories about SSRIS and other psychiatric medications.
Sources:
https://www.mayoclinic.org/diseases-conditions/depression/in-depth/ssris/art-20044825